What are you looking for?
Search

Growth Hormone Deficiency in Children and Peptide Replacement Therapy
ALL ARTICLES AND PRODUCT INFORMATION PROVIDED ON THIS WEBSITE ARE SOLELY FOR INFORMATION DISSEMINATION AND EDUCATIONAL PURPOSES.
The products provided on this website are intended exclusively for in vitro research. In vitro research (Latin: *in glass*, meaning in glassware) is conducted outside the human body. These products are not pharmaceuticals, have not been approved by the U.S. Food and Drug Administration (FDA), and must not be used to prevent, treat, or cure any medical condition, disease, or ailment. It is strictly prohibited by law to introduce these products into the human or animal body in any form.
Overview
Growth Hormone Deficiency (GHD) is a growth and development disorder caused by insufficient secretion or dysfunction of Growth Hormone (GH). GH, a peptide hormone secreted by the anterior pituitary gland, plays a crucial role in children's growth and development. Peptide replacement therapy, as the primary treatment for GHD, has been widely adopted in clinical practice.
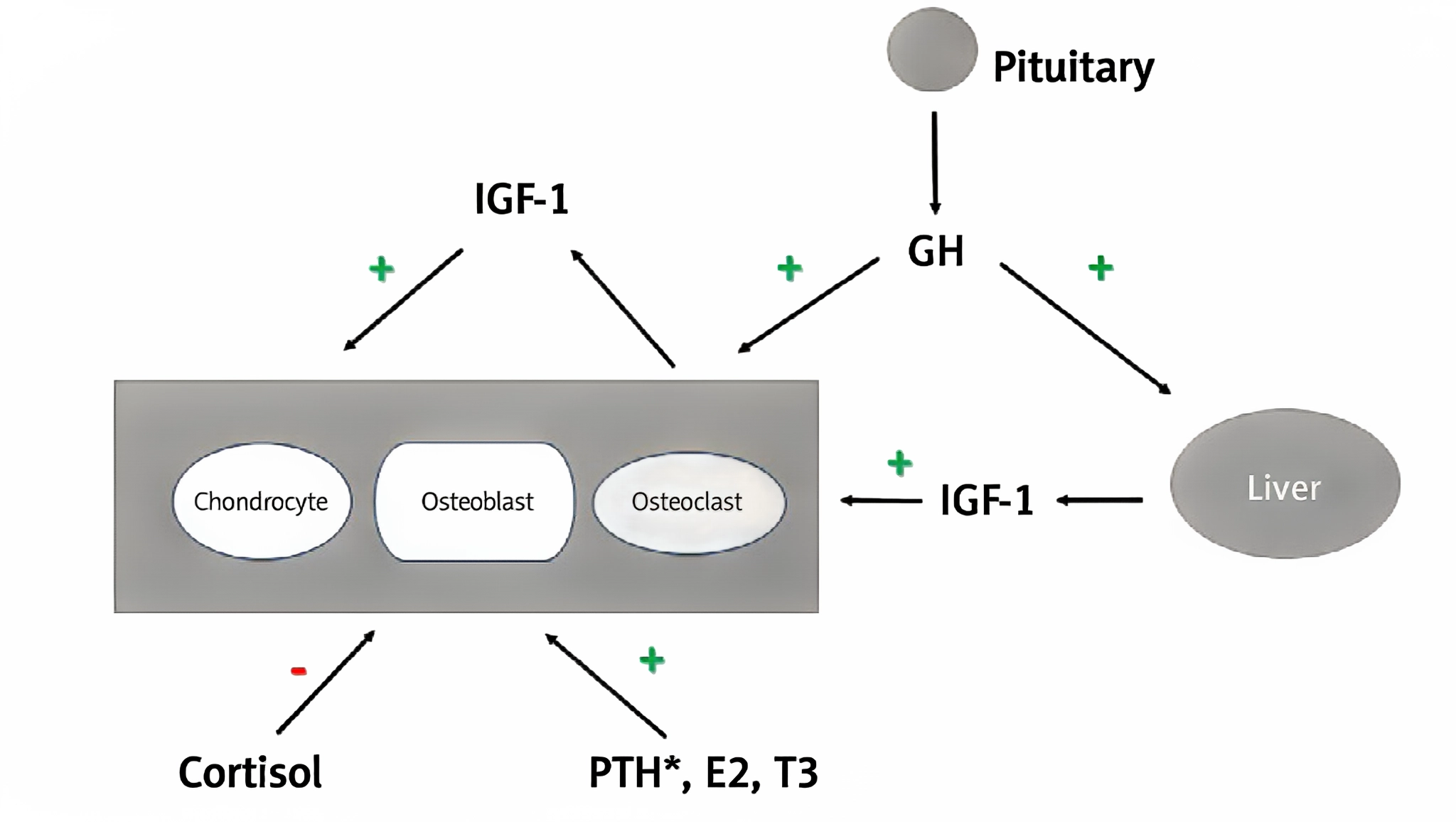
Figure 1 The effect of growth hormone and other hormones on bone.
Physiological Functions of Growth Hormone
(1) Promotion of Growth and Development
Skeletal growth: GH directly acts on the growth plates of bones, stimulating the proliferation and differentiation of cartilage cells, promoting the synthesis and calcification of cartilage matrix, thereby facilitating longitudinal bone growth. For example, during the growth of long bones, GH promotes the continuous division of epiphyseal cartilage cells, increasing the number of cartilage cells, and thereby driving bone elongation.
Organ Growth: GH also promotes the growth of various tissues and organs throughout the body. It stimulates the proliferation of muscle cells and protein synthesis, increasing muscle mass; it promotes the growth and development of internal organs such as the liver and kidneys, maintaining their normal functions. For instance, in muscle tissue, GH upregulates the expression of relevant genes, promoting the growth and hypertrophy of muscle fibers.
(2) Regulation of Metabolic Processes
Glucose metabolism: GH's regulation of glucose metabolism is relatively complex. It can inhibit peripheral tissue uptake and utilization of glucose, leading to elevated blood glucose levels; it can also promote liver glycogen breakdown, further increasing blood glucose levels. Long-term GH action can indirectly enhance insulin sensitivity by promoting the secretion of insulin-like growth factor-1 (IGF-1), thereby lowering blood glucose levels.
Fat metabolism: GH promotes fat breakdown, increasing the release of free fatty acids to provide energy for the body. It also reduces fat tissue accumulation, helping to maintain normal body fat distribution. In some studies, children with growth hormone deficiency (GHD) experienced a significant decrease in body fat content after receiving GH replacement therapy, which is closely related to GH's role in promoting fat metabolism.
Protein metabolism: GH is an important regulator of protein synthesis. It promotes the entry of amino acids into cells, accelerates protein synthesis, and inhibits protein breakdown, thereby increasing the body's protein content. During childhood growth and development, this effect helps maintain the normal growth and repair of tissues such as muscles and bones.
Growth Hormone Deficiency in Children
(1) Pathogenesis
Congenital factors: Some GHD patients are caused by genetic factors. Certain gene mutations can affect GH synthesis, secretion, or action processes. Common genetic defects include mutations in the growth hormone gene (GH1), which can lead to impaired GH synthesis; mutations in genes related to pituitary development, such as PROP1 and POU1F1, can affect the normal development of the anterior pituitary gland, resulting in insufficient GH secretion.
Acquired factors: Acquired factors such as brain tumors, infections, and trauma can also cause GHD. Brain tumors, such as craniopharyngiomas, can compress the pituitary gland or hypothalamus, affecting GH secretion; intracranial infections like encephalitis or meningitis can damage the neuroendocrine cells of the pituitary gland or hypothalamus, leading to abnormal GH secretion; head trauma, especially those involving damage to the pituitary stalk or hypothalamus, may also disrupt the regulatory pathways for GH secretion, leading to GHD.
Idiopathic factors: A portion of GHD patients have no identifiable cause and are classified as having idiopathic GHD. These patients may have mild abnormalities in hypothalamic-pituitary function, but these abnormalities are not severe enough to warrant a definitive diagnosis. It is currently believed that idiopathic GHD may be associated with disruptions in hypothalamic neurotransmitter or neuro-regulatory function.
(2) Clinical manifestations
Growth retardation: This is the most prominent clinical manifestation of GHD. The child's height growth rate is significantly slower than that of peers, with an annual growth rate often less than 5 cm. As the child ages, the height difference from peers gradually increases, and short stature becomes increasingly evident. For example, while normal children grow approximately 5–7 cm per year before puberty, GHD patients may only grow 2–3 cm.
Proportional body build: Although children with GHD are short in stature, their body build is typically proportionate. This differs from familial short stature, where children may exhibit disproportionate limb lengths. Children with GHD often have a childlike facial appearance, with a relatively large head that is disproportionate to their body size. Some children with GHD may also have metabolic abnormalities, such as increased body fat percentage and reduced muscle mass; some may experience delayed sexual development, characterized by delayed onset of puberty and delayed development of secondary sexual characteristics; additionally, children with GHD may have neurological issues such as learning difficulties and attention deficits, which are related to the impact of growth hormone on neurological development.
(3) Methods
Laboratory tests
Growth hormone stimulation test: Since GH is secreted in pulses, random blood sampling to measure GH levels cannot accurately reflect its secretion status. Therefore, a growth hormone stimulation test is required. Commonly used stimulation drugs include insulin, arginine, and clonidine. By administering the stimulation drug, the GH secretion response is observed. Generally, a GH peak below 10 μg/L indicates partial GH deficiency, and a GH peak below 5 μg/L indicates complete GH deficiency.
Insulin-like Growth Factor-1 (IGF-1) and Insulin-like Growth Factor Binding Protein-3 (IGFBP-3) Measurement: IGF-1 and IGFBP-3 levels are closely related to GH secretion and are relatively stable, unaffected by pulsatile secretion. In children with GHD, IGF-1 and IGFBP-3 levels are typically below the normal range for their age. IGF-1 levels are also influenced by factors such as age and nutritional status, so these must be considered comprehensively during diagnosis.
Peptide Replacement Therapy
Drug selection for growth hormone replacement therapy
Recombinant human growth hormone (rhGH): rhGH is currently the most widely used peptide drug for treating GHD in clinical practice. It is produced using genetic engineering technology, with an amino acid sequence identical to that of natural GH. rhGH is available in various formulations, including freeze-dried powder injections and water-based injections. In some studies, the use of recombinant human growth hormone aqueous solutions for treating children with GHD has yielded good therapeutic outcomes, with a significant increase in the rate of height growth in patients.
Long-acting growth hormone: To improve patient compliance, long-acting growth hormone was developed. Long-acting growth hormones are produced by chemically modifying rhGH to extend its half-life in the body, thereby reducing the frequency of injections. Polyethylene glycol-modified recombinant human growth hormone (PEG-rhGH) requires only one injection per week, significantly reducing the injection burden on patients. PEG-rhGH demonstrates similar efficacy and safety to daily injections of rhGH in the treatment of children with GHD.
Research progress on other peptide drugs: In addition to rhGH and its long-acting formulations, several novel peptide drugs are currently under development. For example, certain peptide substances that promote GH secretion or enhance GH action may emerge as new treatment options for GHD.
(2) Treatment Outcomes
Height Gain: Height gain is the most direct indicator for assessing the efficacy of growth hormone replacement therapy. By regularly measuring the child's height, calculating the height growth rate, and comparing it with pre-treatment levels. Generally, within the first 6–12 months of treatment, the height growth rate significantly accelerates, followed by a gradual stabilization. In studies, GHD patients treated with growth hormone for 6 months saw their height growth rate increase from 3 cm per year before treatment to 8 cm per year.
Bone age changes: Bone age is an important indicator of skeletal maturation. Growth hormone therapy may have a certain impact on bone age. During treatment, bone age should be measured regularly to observe the rate of bone age growth. Bone age growth should align with height growth to avoid premature bone age advancement leading to early closure of growth plates, which could affect final adult height.
IGF-1 levels: IGF-1 levels are an important biochemical indicator for assessing the efficacy of growth hormone therapy. Following growth hormone therapy, IGF-1 levels typically increase and are closely correlated with treatment efficacy. Generally, maintaining IGF-1 levels at the upper limit of the normal range or slightly above the normal range indicates good treatment efficacy.
In addition to monitoring changes in physical indicators, the impact of growth hormone therapy on the child's quality of life should also be assessed. This includes the child's psychological state, social skills, and academic performance. After effective growth hormone therapy, the child's self-confidence improves, social activities increase, academic performance improves, and quality of life is significantly enhanced.
Conclusion
Growth hormone deficiency in children is a serious condition that significantly impacts growth and development, with complex underlying mechanisms and diverse clinical manifestations. Peptide replacement therapy, particularly growth hormone replacement therapy, has become the primary treatment for GHD.
Sources
[1] Verrico A, Crocco M, Casalini E, et al. LGG-40. Growth hormone replacement in children on therapy with Vemurafenib for Low Grade Glioma[J]. Neuro-Oncology, 2022,24(Supplement_1):i97.DOI:10.1093/neuonc/noac079.352.
[2] Sävendahl L, Battelino T, Højby R M, et al. Effective GH Replacement With Once-weekly Somapacitan vs Daily GH in Children with GHD: 3-year Results From REAL 3[J]. Journal of Clinical Endocrinology & Metabolism, 2022,107(5):1357-1367.DOI:10.1210/clinem/dgab928.
[3] Caballero-Villarraso J, Aguado R, Cañete M D, et al. Hormone replacement therapy in children with growth hormone deficiency: impact on immune profile[J]. Archives of Physiology and Biochemistry, 2021,127(3):245-249.DOI:10.1080/13813455.2019.1628070.
[4] Wang C, Huang H, Zhao C, et al. The impact of pegylated recombinant human growth hormone replacement therapy on glucose and lipid metabolism in children with growth hormone deficiency[J]. Annals of Palliative Medicine, 2021,10(2):1809-1814.DOI:10.21037/apm-20-871.
[5] Witkowska-Sędek E, Stelmaszczyk-Emmel A, Kucharska A M, et al. Association Between Vitamin D and Carboxy-Terminal Cross-Linked Telopeptide of Type I Collagen in Children During Growth Hormone Replacement Therapy.[J]. Advances in Experimental Medicine and Biology, 2018,1047:53-60. https://api.semanticscholar.org/CorpusID:27770255.
