What are you looking for?
Search

Anti-inflammatory Effects of Bronchogen on Airway Inflammation in Patients with Asthma and Chronic B
ALL ARTICLES AND PRODUCT INFORMATION PROVIDED ON THIS WEBSITE ARE SOLELY FOR INFORMATION DISSEMINATION AND EDUCATIONAL PURPOSES.
The products provided on this website are intended exclusively for in vitro research. In vitro research (Latin: *in glass*, meaning in glassware) is conducted outside the human body. These products are not pharmaceuticals, have not been approved by the U.S. Food and Drug Administration (FDA), and must not be used to prevent, treat, or cure any medical condition, disease, or ailment. It is strictly prohibited by law to introduce these products into the human or animal body in any form.
Overview
(1) Current Status and Risks of Asthma and Chronic Bronchitis
Asthma is a common chronic inflammatory airway disease with a high prevalence worldwide. Its primary characteristics include chronic airway inflammation, airway hyperresponsiveness, and reversible airflow limitation. Patients often experience symptoms such as wheezing, shortness of breath, chest tightness, and coughing, which significantly impair quality of life and may even threaten life. Chronic bronchitis is primarily characterized by chronic nonspecific inflammation of the bronchi, with coughing and sputum production as the main clinical symptoms. The condition persists for at least three months annually for two consecutive years or more.
(2) The Central Role of Airway Inflammation in Asthma and Chronic Bronchitis
Airway Inflammation in Asthma
During the development of asthma, various inflammatory cells such as eosinophils, mast cells, and T lymphocytes are recruited to the airways, releasing a series of inflammatory mediators and cytokines, including interleukin-4 (IL-4), interleukin-5 (IL-5), and interleukin-13 (IL-13), which trigger airway inflammation. These inflammatory responses result in damage to the airway epithelium, increased mucus secretion, airway smooth muscle contraction and remodeling, leading to airway hyperresponsiveness and airflow limitation.
![]()
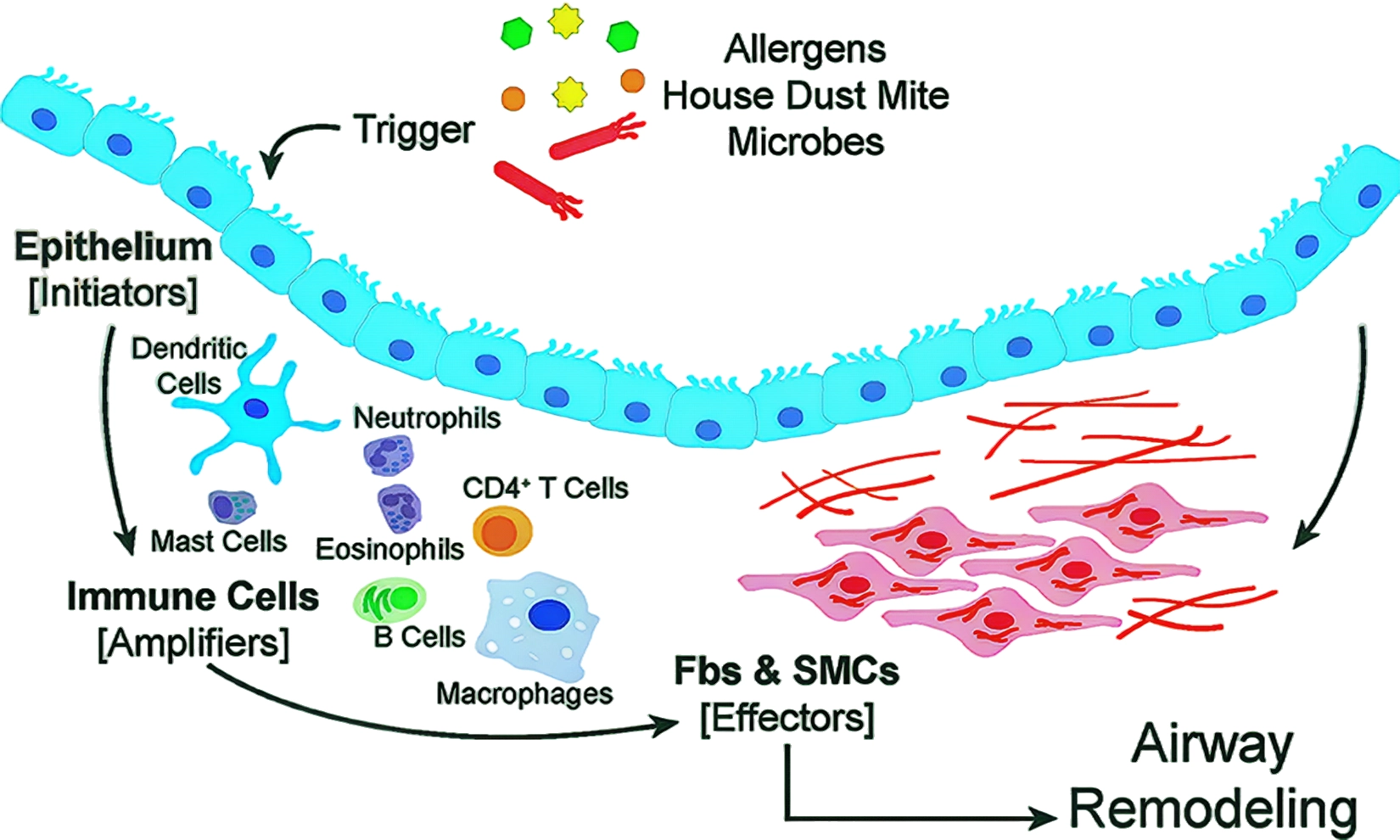
Figure 1 The airway epithelium serves as the primary interface between the environment and the lung.
Airway Inflammation in Chronic Bronchitis
Airway inflammation in chronic bronchitis is primarily mediated by neutrophils, macrophages, and other cells. The proteases, reactive oxygen species, and other substances released during the inflammatory process damage airway structure and function, leading to thickening of the airway walls and narrowing of the lumen, thereby impairing gas exchange. Prolonged inflammatory stimulation can also promote disease progression and increase the risk of complications such as impaired lung function and cardiovascular disease.
(4) Research Background of Bronchogen as a Potential Therapeutic Agent
Given the current state of treatment for airway inflammation in asthma and chronic bronchitis, identifying novel, safe, and effective therapeutic agents holds significant clinical importance. Bronchogen can modulate inflammatory responses through multiple pathways, potentially inhibiting airway inflammation in patients with asthma and chronic bronchitis, thereby aiding in the treatment of these conditions.
The Inhibitory Effect of Bronchogen on Airway Inflammation in Asthma Patients
(1) Regulatory Effects on Inflammatory Cells
Eosinophils
Eosinophils play a key role in airway inflammation in asthma. The toxic substances they release, such as eosinophil cationic protein, can damage airway epithelial cells and exacerbate inflammatory responses. Bronchogen can inhibit the chemotaxis and activation of eosinophils, reducing their infiltration into the airways. By regulating the expression of chemokine receptors, specifically CC chemokine receptor 3 (CCR3), it blocks the adhesion between eosinophils and airway epithelial cells as well as endothelial cells, thereby reducing their aggregation in airway tissue.
T lymphocytes
Th2 cells are important immune cells in asthma inflammation, secreting cytokines such as IL-4, IL-5, and IL-13, promoting eosinophil activation and airway hyperresponsiveness. Bronchogen inhibits Th2 cell differentiation and function, reducing the production of these cytokines. Bronchogen also regulates the number and function of regulatory T cells (Tregs), enhancing Tregs' inhibitory effect on Th2 cells, maintaining immune balance, and alleviating airway inflammation.
Mast cells
Mast cells rapidly release inflammatory mediators such as histamine and leukotrienes during asthma attacks, triggering airway smooth muscle contraction and increased vascular permeability. Bronchogen stabilizes mast cell membranes, inhibits degranulation, and reduces the release of inflammatory mediators, thereby alleviating acute airway inflammation.
(2) Effects on inflammatory mediators and cytokines
Reducing the release of inflammatory mediators
In addition to inhibiting the release of histamine and leukotrienes from mast cells, Bronchogen also reduces the levels of other inflammatory mediators, such as prostaglandin D₂ (PGD₂) and thromboxane A₂ (TXA₂). These inflammatory mediators can cause bronchial smooth muscle contraction, increased mucus secretion, and vasodilation, exacerbating bronchial inflammation. By inhibiting the activity of enzymes such as cyclooxygenase (COX), Bronchogen reduces the synthesis of PGD₂ and TXA₂, thereby alleviating bronchial inflammatory responses.
Regulation of the Cytokine Network
As mentioned earlier, asthma patients exhibit imbalances in various cytokines within the airways, with elevated levels of Th2-type cytokines such as IL-4, IL-5, and IL-13, while anti-inflammatory cytokines like IL-10 are reduced. Bronchogen can upregulate the expression of anti-inflammatory cytokines such as IL-10, while inhibiting the production of pro-inflammatory cytokines such as IL-4, IL-5, and IL-13, thereby correcting cytokine network imbalances and reducing airway inflammation. Bronchogen also inhibits the activity of cytokines such as tumor necrosis factor-α (TNF-α) and interferon-γ (IFN-γ), which also play important roles in asthma airway inflammation and airway remodeling.
![]()
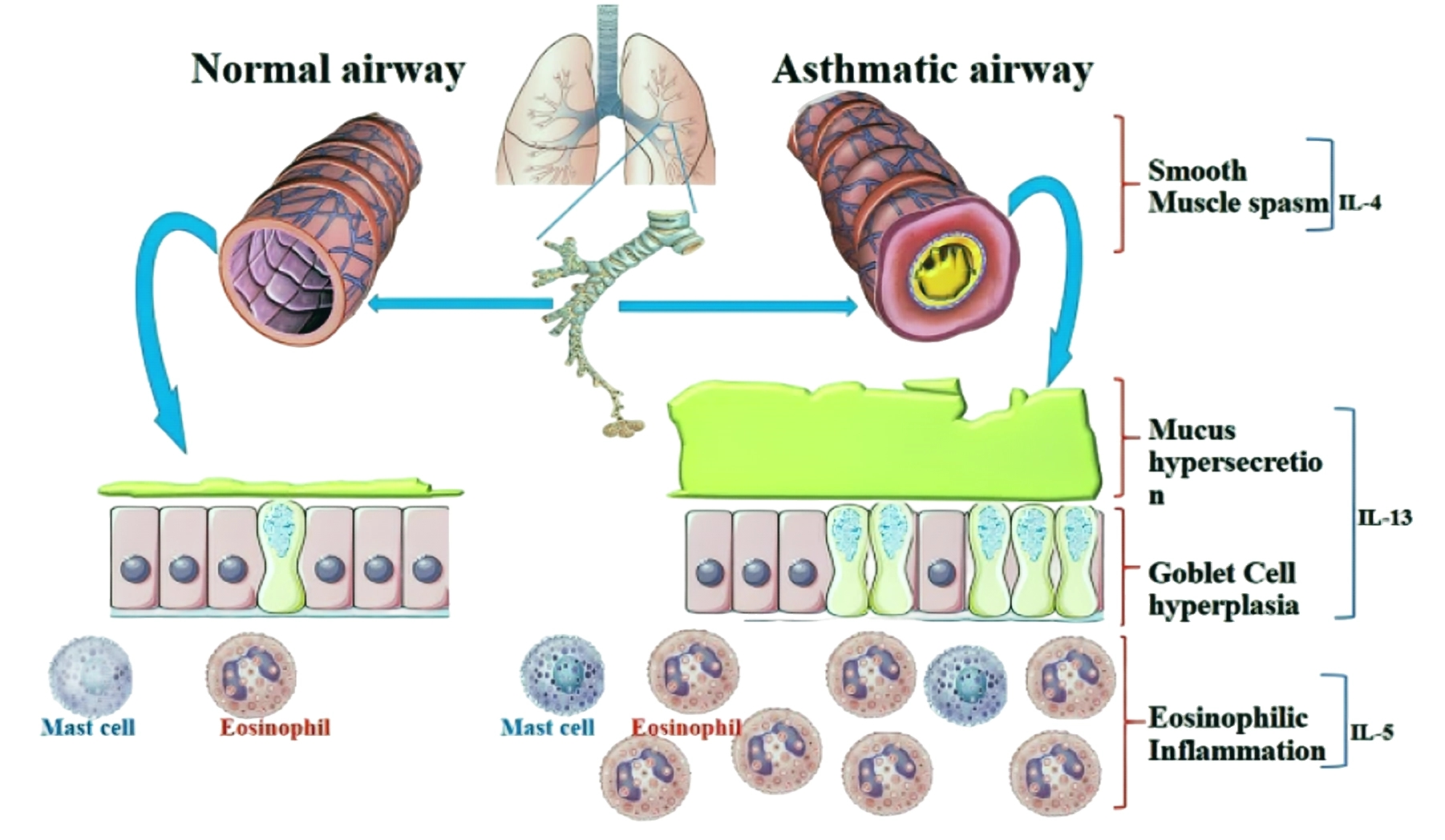
Figure 2 Asthma, a chronic inflammatory airway disease, is characterized by eosinophilic inflammation, mucus hypersecretion, goblet cell hyperplasia, airway hyper-responsiveness, and breathlessness.
(3) Protective effects on airway epithelial cells
Reducing epithelial cell damage
Asthma airway inflammation can lead to damage to airway epithelial cells, impairing the airway barrier function. Bronchogen promotes the repair and regeneration of airway epithelial cells, enhancing their barrier function. Bronchogen upregulates the expression of tight junction proteins such as occludin and tight junction protein-1 (ZO-1), maintaining tight junctions between epithelial cells and reducing the influx of inflammatory mediators and allergens.
Inhibition of excessive mucus secretion
Excessive mucus secretion in the airways is one of the key pathological features of asthma. Excessive mucus can obstruct the airways and exacerbate airflow limitation. Bronchogen reduces mucus synthesis and secretion by inhibiting the expression of mucin (MUC) genes in airway epithelial cells. Additionally, it regulates mucociliary clearance function, promoting the removal of mucus from the airways and maintaining airway patency.
(4) Effects on airway remodeling
Inhibiting smooth muscle cell proliferation and migration
Airway remodeling is an important pathological change in asthma, including thickening of airway smooth muscle and deposition of extracellular matrix. Bronchogen inhibits the proliferation and migration of airway smooth muscle cells, reducing their number and volume. By regulating the expression of cell cycle-related proteins, cyclin-dependent kinases (CDKs), and cyclins, Bronchogen causes airway smooth muscle cells to arrest at specific stages of the cell cycle, thereby inhibiting their proliferation.
Reducing extracellular matrix deposition
During asthma airway remodeling, fibroblasts synthesize and secrete excessive amounts of extracellular matrix components such as collagen and fibronectin, leading to thickening of the airway walls. Bronchogen can inhibit the activation and proliferation of fibroblasts, reducing the synthesis and deposition of extracellular matrix components. It can also regulate the balance between matrix metalloproteinases (MMPs) and their tissue inhibitors (TIMPs), promoting the degradation of extracellular matrix and alleviating the extent of airway remodeling.
Bronchogen's inhibitory effect on airway inflammation in patients with chronic bronchitis
(1) Regulation of inflammatory cell recruitment and activation
Neutrophils
Neutrophils dominate airway inflammation in chronic bronchitis, and the proteases they release, such as elastase, can damage airway structure. Bronchogen can inhibit neutrophil chemotaxis and activation, reducing their accumulation in the airways. By inhibiting the expression of integrins on the surface of neutrophils, such as β₂ integrin, it reduces the adhesion of neutrophils to endothelial cells, thereby decreasing their migration into airway tissues.
Macrophages
Macrophages not only participate in pathogen clearance during the inflammatory process of chronic bronchitis but also release various inflammatory mediators. Bronchogen can regulate the polarization state of macrophages, promoting their transformation into anti-inflammatory (M2-type) macrophages, thereby reducing the release of pro-inflammatory cytokines such as IL-1β and TNF-α while increasing the secretion of anti-inflammatory cytokines such as IL-10, thereby alleviating airway inflammation.
(2) Effects on Inflammatory Mediators and Proteases
Reducing Inflammatory Mediator Levels
In patients with chronic bronchitis, various inflammatory mediators are elevated in the airways, such as IL-8 and leukotriene B₄ (LTB₄). These inflammatory mediators attract neutrophils and other inflammatory cells, exacerbating the inflammatory response. Bronchogen can inhibit the production and release of these inflammatory mediators by suppressing the activation of inflammatory signaling pathways such as nuclear factor-κB (NF-κB), thereby reducing the gene transcription and synthesis of inflammatory mediators.
Inhibiting protease activity
Proteases released by neutrophils, such as elastase and cathepsin, can degrade elastic fibers and collagen in the airways, leading to damage to the airway walls. Bronchogen has protease inhibitory activity, directly inhibiting the activity of these proteases and reducing damage to airway tissues. It can also regulate the balance between proteases and their inhibitors, increasing the levels of protease inhibitors such as α₁-antitrypsin, further alleviating protease-induced damage to the airways.
(3) Improvement of airway mucus hypersecretion and ciliary function
Reduction of mucus secretion
Patients with chronic bronchitis often experience increased mucus secretion in the airways, exacerbating coughing and sputum production. Bronchogen can reduce mucus synthesis and secretion by inhibiting the expression of the MUC gene in airway epithelial cells. It can also regulate the physicochemical properties of airway mucus, reducing its viscosity and making it easier to expel.
Enhancing ciliary function
Normal ciliary movement in the airways is a key mechanism for clearing airway secretions. In patients with chronic bronchitis, impaired ciliary function leads to mucus clearance. Bronchogen promotes the repair and regeneration of airway ciliated cells, enhancing ciliary beating frequency and amplitude, thereby improving mucociliary clearance function. This aids in the expulsion of secretions and pathogens from the airways, alleviating airway inflammation.
(4) Protection of airway structure and function
Reducing airway wall thickening
Chronic airway inflammation can lead to thickening of the airway walls and narrowing of the lumen in patients with chronic bronchitis. Bronchogen reduces the extent of airway wall thickening by inhibiting the infiltration of inflammatory cells, reducing damage from inflammatory mediators and proteases, and regulating the metabolism of the extracellular matrix, thereby maintaining the normal structure and patency of the airways.
Improving lung function
By reducing airway inflammation, decreasing mucus secretion, enhancing ciliary function, and protecting airway structure, Bronchogen helps improve lung function in patients with chronic bronchitis. Studies have shown that after treatment with Bronchogen, patients' lung function parameters such as forced expiratory volume in one second (FEV₁) and forced vital capacity (FVC) significantly improved, and symptoms such as dyspnea were markedly alleviated.
Conclusion
In summary, Bronchogen, as a potential drug for treating airway inflammation in asthma and chronic bronchitis, possesses a multi-targeted, multi-pathway anti-inflammatory mechanism of action. By regulating inflammatory cells, inflammatory mediators, airway epithelial cells, and airway remodeling, Bronchogen effectively suppresses airway inflammation in asthma and chronic bronchitis patients, improves airway structure and function, and enhances patients' quality of life.
Sources
[1] Son J W, Lim S. Glucagon-Like Peptide-1 Based Therapies: A New Horizon in Obesity Management[J]. Endocrinology and Metabolism, 2024,39(2):206-221.DOI:10.3803/EnM.2024.1940.
[2] Hough K P, Curtiss M L, Blain T J, et al. Airway Remodeling in Asthma[J]. Frontiers in Medicine, 2020,Volume 7.DOI:org/10.3389/fmed.2020.00191.
[3] Athari S S. Targeting cell signaling in allergic asthma[J]. Signal Transduction and Targeted Therapy, 2019,4(1):45.DOI:10.1038/s41392-019-0079-0.
Product available for research use only:
![]()

